


The Billion Dollar Baby and the Billion Dollar Question- The Fauci great grift & hoax implemented on the world to allow Fauci/Moderna to gain EUA approval for LNP-mRNA technology.
The mRNA "Vaccine" money trail, players, playbook, shell game, and "miraculous" Emergency Use Authorization (EUA) for the technology that struggled to gain approval for twenty years pre-pandemic.

The Billion Dollar Baby: And The Billion Dollar Question
A Deep Dive into the EUA Vaccine Roll-Out and The Money Trail
Written by Heather Hudson
A Call to Action:
Most who will read this article know that I am the mother of a young adult son who was significantly injured by his mRNA Covid-19 “vaccine” (AKA jab, shot, or therapy). Most do not refer to gene therapy as a "vaccine,” as it was not a vaccine, and beacuse of this, for most of this article I becausewill use the “v” word in quotes.
This is the story of The Billion Dollar Baby - AKA the LNP and mRNA technology, a struggling pre-pandemic technology that was only approved via the Emergency Use Authorization (EUA). Here, we take a deep dive, questioning everything to do with the years-long lead-up to its blatantly irregular and questionable EUA approval.
We take a look at certain aspects of the Billion dollar Baby’s money trail, the players, and the playbook that allowed this otherwise cautioned-against technology to gain approval in the chaotic pre-pandemic and pandemic world of newely generated public agencies, grants, and nepostism, and select “players” that set-up the “poised-perfect-solution,” ready and waiting for the “perfect pandemic” to come along, “authorizing” billions of dollars in expected profits for this technology and all the parties that were set in place to ensure everything went according to the pre-pandemic plan.
Our “pandmedic” story begins with Cody’s story, which can be seen in my SubStack first in the article The Shot Heard Around the World or other articles that I will write or that feature his Covid-19 mRNA vaccine injury and the injuries of others as we advocate for others and seek treatments and the best possible outcome for Cody. Where applicable, here in The Billion Dollar Baby, I will provide information about his medical case for context.
Cody’s injury is the reason why I write about the pandemic, medical injustice, the EUA drugs and Covid-19 “vaccine” adverse events and pandemic medicine.
My direction and my son’s direction in life changed drastically after his second Covid-19 mRNA injection. My son spent his 22nd birthday hospitalized with a large pulmonary embolism, blood clotting, neuropathy, skin lesions, leaky heart valves, left ventricular hypertrophy, significant right-side weakness, and bleeding lungs. He entered the hospital at age 21 and left after his birthday, barely breathing and unable to walk on his own since then.
He spent about seven months without care for his blood clotting disorder, gasping for breath and clinging to life as hospitals and doctors dismissed him throughout our region as I attempted to find a doctor who would treat him. His case is profound and can be found online. It describes a documented case of vaccine injury.
After fourteen months (late 2022), he is left with antiphospholipid syndrome, a life-threatening blood clotting disorder, neuropathy, skin lesions, and weakness. He is 23, walks with a cane, and takes six prescription medications.
My son, his doctors, and I have talked about his case and the vaccine adverse events in programs in the US and Canada, and we have helped vaccine-injured citizens in the UK, the US, and Canada through advocacy. We are meeting more and more vaccine-injured people, and we have found that our work and voice are not alone. An army of volunteers and families like ours have had their lives halted by the Covid-19 “vaccines.” We have all stepped forward to bring the truth to light.
In April 2022, as my son began to get genuine treatment for his blood clotting disorder, even though he was significantly ill, I began to research the Covid-19 mRNA lipid shell in order to find what could have caused such a systemic and life-threatening event in my son’s body. I could not let another parent or child go through what he had gone through.
My research on the mRNA lipid shell, LNPs, PEG, PEGylated lipids, and liposomes made the world stage when a world-renowned doctor and former consultant for the WHO (World Health Organization), who specialized in evaluating research for them for ten years, published my work in October 2022.
Again, my world changed in a heartbeat. I had already been writing about these issues with a dedicated physician before this fateful event. Still, we were doing this work on our own, trying to fight the tide of a broken medical system and witnessing significant censorship of long-known, long-approved medical practices and treatments.
But after finding a voice on a bigger stage, physicians and support from members of the medical community around the world began to surround my efforts and my son’s bravery and his voice.
While watching over my son and watching him slowly recover to whatever point his body will eventually recover, I have kept my nose to the research and writing as it is apparent with the global pandemic policy failures, failing trust in our medical community, and prescription drugs safety, that a revolution and a call for change has begun.
I believe that the way that prescription medication is approved, chosen for approval, and determined safe for consumer use is on the way to a new future, and these vital steps in medication safety will be taken out of the hands of mega public medical figures. Even if most “mainstream” news and “mainstream” citizens don’t know it yet, trust in our medical leaders “hit a wall” for the rest of us, and the resounding call to action to find a better way is being heard and felt like a bass drum’s percussion through the world of medicine.
Due to the failures of these regulatory agencies, pushing and allowing known dangerous technology on our citizens my son developed antiphospholipid syndrome, (one of the most severe and insideous versions of the disease) and the phospholipids in the Covid-19 mRNA “vaccines” or therapy were coated in known toxins, which his body did not recognize and mistook his own phospholipids as “enemies” or, “non self” he developed this life-long and likely terminal autoimmune blood clotting disorder.
Countless others fell ill from neurological, blood clotting, autoimmune and cardiac adverse events linked ot the “vaccines.”
To prevent other families, children and people from experiencing this nightmare, I also began to look at how this LNP-mRNA “vaccine” “therapy” was approved for a “one-size-fits-all” therapy on a global scale in a global “vaccine” campaign.
These hurting families and my son’s heart-wrenching case brought me to research the lipid shell, the pre-pandemic liposomes, LNP development, and the role of the lipids in the Covid-19 vaccines. I write about Covid-19 vaccine adverse events and pandemic injustices.
In this, I also researched alternatives to the Covid-19 vaccines and Covid-19 alternative therapies, this included ivermectin and hydroxychloroquine, but I also explore some of the other lesser-known alternatives that are being used in the viral labs.
These are alternatives that should have been considered and researched if it were not for the Billion Dollar Baby (the Covid-19 vaccine technology) that was pre-determined long ago to make it to the EUA finish line, while all other alternatives were “knee-capped” by the public health agencies.
The Lie:
I first looked at the EUA (Emergency Use Authorization) to question why and how the lipids, emulsifiers LNP-mRNA therapies were allowed to obtain EUA approval given their track record, which kept them from the ability to progress to the point of approval in the past (pre-pandemic) and would not have allowed the FDA-granted approval without an “emergency” or “pandemic” to “necessitate” the EUA measures and capitulations seen in the early pandemic. Well, in the early pandemic and long before that.
After reading and researching the events that allowed this to happen, I and countless others began to question whether other safer drugs may have been “canceled” or passed over potentially for the Covid-19 vaccines to be approved.
It quickly became clear to me that it was not just the attacks on the safe and well-known drugs like ivermectin and hydroxychloroquin that took place to set the approval in motion for the Covid-19 vaccines -or more specifically- to set the LNP-mRNA gene therapy technology in motion for approval.
Although insideous, there is so much more to the story than the attempts to decimate the use of ivermectin and hydroxychloroquine. The money trail, the grants, and the birth of new public health agencies began in the early 2000s, and the story of the questionable lipid technology starts long before that.
The mRNA and pseudouridine story also ties into these pre-pandemic failures, and later, I will write about the dangers therein and the challenges this facet of the technology faced pre-pandemic.
But for now, I will focus on the EUA approval of this previously struggling technology and how the Billion Dollar Baby was born with the development of the EUA that was so obviously intended to bring to life- a previously DOA technology.
This is a story right out of nightmares and the era of Frankenstein’s monster disguised as a zippy campaign “for the greater good” complete with synchronized dancers.
Although some will forever want to ignore these adverse events and the possibility that millions were harmed for a gene therapy technology -which struggled for approval and was cautioned against by many in the medical field- to obtain Federal Drug Agency approval, on an “emergency” basis, we must speak honestly and openly as a society about these horror-movie-esque details to get to a place where we gain more transparency and are not put in the position to be deceived in matters surrounding our health and the government’s role in harming citizens.
We all learned from reading the pandemic public health policies that Emergency Use Authorization (EUA) for the “vaccines” could not take place if alternative (or other) drugs were available that met the need for efficacy and safety criteria in treating Covid-19 infections.
Simply put, there would be no need for an Emergency Use Authorization for the Covid-19 vaccines and no need for the rushed Covid-19 vaccines if the government had recognized that drugs, treatments, or therapies were available to protect from or treat Covid-19 infection or SARS-CoV-2 virus.
Many of you may know this, but many may not, so I will give this FDA information here for reference.
“An Emergency Use Authorization (EUA) is an FDA mechanism to facilitate the availability and use of medical countermeasures, including vaccines, during public health emergencies, such as the current COVID-19 pandemic. Under an EUA, the FDA may allow the use of unapproved medical products or unapproved uses of approved medical products in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions when certain statutory criteria have been met, including that there are no adequate, approved, and available alternatives. Taking into consideration input from the FDA, manufacturers decide whether and when to submit an EUA request to FDA.
Once submitted, FDA will evaluate an EUA request and determine whether the relevant statutory criteria are met, taking into account the totality of the scientific evidence about the vaccine that is available to FDA.” Found on the FDA’s website under “Emergency Use Authorizations Vaccines.”
Truth Does Not Mind Being Questioned:
What if new medications and a “warp speed” vaccine weren’t needed to combat this novel Coronavirus? What if a “Billion Dollar Baby” were the bigger picture of what caused our country significant chaos and harm?
If we face the reasons behind the pandemic public health agency calamity, we will know what answers to demand when Congress investigates. If we look away, we will surely be in the midst of this chaos and tyranny again.
Recently, Steve Kirsch wrote on his Substack, “Truth does not mind being questioned; a lie does not like being challenged.” Please keep this in mind as you read on.
I write and research pandemic injustices, medical policy failures, and other issues with doctors, nurses, and advocates who were Frontline Covid-19 medical workers before there were sanctioned and EUA treatments. At the time, no guidelines were set for treatment by the FDA, NIH, CDC, etc. Tens of thousands of doctors did this work when others stepped back.
Over the months, I interviewed some of the most severe Covid-19 patients in Florida and reviewed their medical cases. The takeaway from what I learned from working with Frontline doctors and from reading about the work of multitudes of frontline medical professionals is this fundamental concept that is often overlooked: Covid-19, for the most part, is highly treatable; it is a virus, and the symptoms can be treated with therapies that were readily available before the EUA drugs and vaccines were approved..
Most doctors who treated COVID-19 patients before there were public health “guidelines or treatments” decreed by federal and international “authorities” are now writing about these experiences. Sadly, this has taken bravery as many of them risk losing their positions, licenses, or credibility when they tell others that Covid-19 is treatable and that there is no need for EUA-mandated drugs or a Covid-19 “vaccine.” These doctors questioned the lies.
But how do they know Covid-19 SARS-CoV-2 is treatable? They are doctors, and they are trained to treat illness and injury presented to them -as they have always done.
They look at the symptoms, just like they do when they don’t know what is ailing a patient, then run tests to see the severity of those ailments and treat them accordingly. Again, I know this as I write with doctors who have written these words with me and made Covid-19 presentations along with me.
Inflammation, fever, nausea, and cough are all symptoms that doctors already treat. Patients and doctors worldwide are now speaking out to describe their experiences with existing treatments for even the more severe cases, with blood clotting and pneumonia.
Tens of thousands of frontline doctors did this work when the government claimed there were “no treatments.” The frontline doctors saw ailments they have been treating their entire careers (inflammation, pain, cough, pneumonia, etc.) using known treatments, and their patients survived.
They used typical tools that doctors use to detect more severe cases, including bloodwork and diagnostic testing, which all tell the doctor a story of the needed care and treatment of the patient.
Sadly, many patients died from Covid-19 in hospital settings as they were told by doctors who were not treating Covid-19 patients to go to the hospital only when their case was severe.
Waiting meant the illness had time to worsen, and it also meant the patients went to hospitals that independent frontline doctors did not staff. These very ill patients were then in the hands of physicians who answered to insurance companies, medical boards, and pandemic protocols developed by the public health agencies (who were not doctors treating the Covid-19 patients).
Independent thinking was discouraged in the mainstream hospitals and hospital systems. Almost always, these hospitals prevented their doctors from using alternative treatments when the mandated treatments weren’t working, and patients died- countless patients died.
Articles can be found online about patients seeking alternative treatments, such as hydroxychloroquine or ivermectin. These treatments worked for the frontline doctors, but the hospitals would not allow them.
The hospital protocols dictated the use of EUA drugs (which were limited) and the approved drugs on the FDA’s temporary policy page, which are primarily heavy sedatives/anesthesia drugs and painkillers -not all, but most- see below.
Additionally, these protocols had financial ties to the well-known Covid-19 HHS CARES Act hospital incentives and insurance funding. The adherence to the protocols also had career implications that could influence the livelihood of the doctors if they did not use them.
Reading it and hearing it sounds extreme because it is extreme. Our nation’s health care system was and is extremely broken by these practices.
The FDA’s “temporary policy” list of the drugs that received EUA approval is provided here. I found the drugs on this list to be primarily sedatives and potent painkillers like Fentanyl and Ketamine. It also included a strong antibacterial drug (Vancomycin) and two blood pressure drugs as seen here: List of Drugs Used for Hospitalized Patients with COVID-19, December 2021: https://www.fda.gov/media/138276/download
Outside the hospitals, the frontline doctors continued successfully treating their Covid-19 patients with readily available, safe, and effective drugs that had been around (for many of them) for most of their careers.
However, using effective and long-used drugs such as ivermectin and hydroxychloroquine, antibiotics, and anti-inflammatories threatened the potency and validity of the EUA. Again, if “safe and effective” drugs were known to successfully treat Covid-19 (such as what the frontline doctors were seeing), then the EUA drugs and the Covid-19 vaccines could not be authorized.
The attack campaigns on these drugs were unprecedented and misled millions into thinking that successful and long-known treatments were dangerous.
But wait… there’s more. Much more.
Lying by acts of omission:
For those who are reluctant or are outright afraid to open their eyes to the possibility that we were duped by the public health decress and attacks on the long-known safe drugs and medications in order for the government to authorize remdesivir and other hospital protocol drugs that are dengerous, and to authorize the Covid-19 vaccines, below are a sampling of the track record of misconduct and lack of integrity found within our nation’s largest public health organizations and drug manufacturers. There are many more.
I’ll start with the story of Brook Jackson, a woman with nerves of steel. I know Brook’s story, and many people know Brook’s story, and more people will learn the details about her story as time goes on. But what is astounding is that the FDA didn’t seem to want to know Brook’s story.
Brook is a whistleblower who worked at one of the Pfizer Covid-19 vaccine trial sites. She saw irregularities and reached out to authorities, like all citizens are asked to do “see something, say something.” This is what Brook did to attempt to ensure that the American people were getting a safe product. Since then, she has been stonewalled, stalled, and jerked around in her quest to have her knowledge of data integrity issues in her work with the Pfizer Covid-19 “vaccine” clinical trials looked at objectively.
In attempting to do this, she has been wronged by no less than the FDA, according to a letter from the offices of the OCI, obtained by Maryanne Demasi of the Epoch Times in her December 7th, 2022, article:
“On Nov. 2, 2021, The BMJ broke the story of Brook Jackson, the regional director who blew the whistle on data integrity issues in Pfizer’s pivotal COVID-19 vaccine trial. Weeks later, documents were leaked supporting Jackson’s complaint about “falsified data.”
“Among the leaked documents was an email, authored by a former federal agent in the FDA’s Office of Criminal Investigations (OCI), claiming Pfizer knowingly submitted fraudulent data to the FDA, and the agency responded by turning a blind eye… To grasp the gravity of what is written in the email, it’s important to understand the role of OCI.”
In Maryanne Demasi’s article (linked below) on the offices of the OCI (OCI is the FDA’s criminal law enforcement arm), “The unit was established by former FDA Commissioner David Kessler, off the back of the generic drug scandal in the late 80s. Kessler was determined to crack down on fraud after FDA employees were found guilty of accepting bribes from generic drug makers.
The story continues, “What I care about most is restoring the credibility and the integrity of the Food and Drug Administration,” said Kessler at the time,” and the only way to do that is to focus on strong enforcement. We are going to enforce the law.”
“Since then, many OCI investigations have led to arrests, hefty fines, and imprisonment, such as the recent [2022] sentencing of two clinical trial researchers in Florida for conspiracy to falsify data by making it appear as though subjects were participating in the trials when, in truth, they were not.” Found in the article, FDA ‘Turned a Blind Eye’ to ‘Submission of Fraudulent Data’ on COVID Vaccine, Says Former Criminal Investigator - Pfizer and FDA respond to leaked OCI email https://www.theepochtimes.com/health/fda-blind-eye_4901497.html
For those agencies who take part in these questionable activities and for them to also make a mockery of FDA-approved medications that were acceptable and used for more than thirty years pre-pandemic without large-scale safety concerns, along with the past prosecuted misconduct documented by the DOJ; Who regulates the regulators and why aren’t they doing so now?
These details all speak to a bigger story. Where is Congress and the Senate in all of this and will they do more than develop reports on these issues?
Follow the Money:
The pandemic failures and inactions on the part of our regulatory agencies and Congress and Senate beg the question, where is the money in all of this? Who got paid?
If we follow the money, the “vaccines” and, more specifically, the Covid-19 mRNA “vaccine” lipid shell delivery system (and platform) were the highest-priced commodities in the pandemic (detailed within this article).
Each aspect of these issue of payments to agencies and politicians should be looked at carefully. It should not sit right with us. People are still dying despite billions of money to “CARE” for them!
At this point of the pandemic, many understand something went terribly wrong, as after these multi-billions of dollars in global efforts, and after nearly three years, illness, injury, and death are still prevalent.
What is most troubling aspect in this is that the “solution,” the “vaccines” that were made to “calm” this virus or “flatten the curve” in our population, is instead making people sick and die, including the near death of my son, who is still fighting for his life.
So we must look at the fincial details and the origins of the virus (which is now taking place in hearings), the relationships, actions, inactions, money and motivations of the agencies that took charge, and the hospital “treatments” and “vaccines” they developed and used to “clean up the virus.”
We must follow the money and refrain from taking the easy way out. We have to stop looking at the idea that our government can do these insidious things as a fringe ideas!
In turn, we must also stop trusting agencies that won’t look into whistleblower claims and listen to world-renowned physcicians in a global health crisis.
These agencies admit and detail the wrongdoings and injustices that take place within their own walls often, and most government agencies have internal affairs offices and special prosecutors to prosecute their “own people” when they break the law in their roles. We must face these facts head-on. These internal affairs offices are there to protect us from those who should be protecting us!
Many may find it hard to read or accept that our medical leaders were misguided or, worse, getting kickbacks or promised or potential promotions in these seedy efforts. The facts are that most people lost faith in medicine and medical leaders during the pandemic, but still, not enough are investigating with the fury that most should possess over these deaths and the multi-billions of wasted tax dollars!
These are the hard-earned dollars of American workers that were spent to “guide” us through this, but instead left us with chaos in our medical system and federal public health agencies, and of course death tolls and injured that won’t be fully accounted until years from now.
This article is an attempt to highlight and bring a lens over these hard facts to bring the details into focus so that we know exactly what was done so lives can be saved as we are clearly continuing to see deaths.
We also need to know precisely what to investigate, as spinning our wheels as a nation in circus-like hearings and investigations will only bring about further chaos and distrust to an already weary world that is in disbelief of the idea that these “leaders” can get away with what has been done.
Let that serve as a warning. Investigations need to begin now.
A Lie Does Not Like Being Challenged:
Details can be hard for most people to look at as they often highlight what we don’t want to see. For instance, most of us have no desire to look at the dust from our nightstand under a microscope when cleaning. We don’t want to think about little organisms in the dust, and as we clean it up, many don’t pay much attention to the cleaner we use to remove it. The detailed ingredients and chemicals in the cleaner might be worrisome if we looked closely enough. For most, it is enough to know we removed the dust and cleaned the nightstand.
The idea that we may have caused more harm with the cleaner than the dust’s presence is a good example of what has taken place in the pandemic as the cure, “vaccines,” seem as if they may be more harmful than the virus at this point and if one listens to physicians that are brave enough to speak the truth.
We know that details are hard to look at for those who are starting to realize that something with this entire pandemic scenario isn’t right. But for those who lost loved ones, jobs, homes, etc., the details are vital now, so we have to make an effort to get to the bottom of it.
In a hypothetical scenario, what if, out of caution, you had a cleaning company clean the dust with a newly marketed cleaning solution? What if, after this, the people in your home started becoming sick or even suffered a life-threatening illness?
What if many others hired this same cleaning agency to clean, and those families also fell deathly ill?
If this happened in real life, the dust, cleaning agency, and cleaning solution would likely be investigated with a forensics-level investigation needed to prevent further illness and death (very similar to how the EPA investigated Legionnaires disease or the CDC investigates when people fall ill from salmonella in foods like lettuce).
However, no mass-scale investigation has taken place yet with the Covid-19 “vaccine” injuries, the policies, and the “leadership” that brought about the “vaccines” and left a crucial aspect of looking into illness after the vaccines out of the equation -during a global “vaccine” campaign!.
This is tragic, and my wish is that the Covid-19 injections were halted now, but if they aren’t stopped yet, possibly the only good thing about that is that the people working towards exposing the whole story can move the talking point to the long-term danger: the LNP and platform that will remain in future drugs. We can’t just ask for the Covid-19 injections to be stopped. We must ask for the injections and the LNP shell (and platform) to be stopped as well.
Deadly Distraction:
When the truth begins to unravel, the litigators, politicians, and pundits may get a false sense of altruism and allow themselves to chase the deadly distraction or token gesture if drug manufacturers and developers begin to declare that it was the spike protein alone causing the vaccine injuries and adverse events.
We may see this in the years to come as we pursue them in what I believe I see as their failures and frauds. If our attorneys are clever enough, the drug makers may promise change and then focus their “improvement” on the payload only (the spike protein), thereby ignoring the issues with the LNP and mRNA or contaminants altogether. Or they may decide that their “research “confirms” that any reaction to do with the lipid shell is an allergic reaction alone.
People do not have to be allergic to PEG or the LNP ingredients to die from them or to be significantly injured by them or killed by them.
To be clear, the platform (the shell) is dangerous and will be used in injections for the next 15 or so years. The lipids have a known history of harms and concerns about the mRNA technology can be seen in studies and the 2020 and 2021 EMA Comirnaty vaccine report and in peer-reviewed studies and articles since the roll-out of the vaccines.
Pre pandemic LNP and mRNA technology studies are referenced are found in many of my SubStack articles. Again, I this is why I focus on the lipids and platform.
Yes, the spike protein has known and documented adverse reactions. But if we don’t address all the potential adverse events, our children will have the dangerous LNP shells, lipids, emulsifiers, pseudouridine-modified RNA, or similar platform formulations that can cause identical and similar adverse events in their vaccines or gene therapies.
These adverse reactions have been seen not only in the Covid-19 injections, but they have been known to take place years before the pandemic in the “similar” lipids used in lipid delivery drugs that had life-threatening reactions that are attributed to the lipids and are NOT solely allergies. Allergies are only one potential reaction path.
The other known reactions or adverse events can take place without warning and are not allergies; in fact, they are called pseudoallergies, which can be life-threatening, mild, or fatal. They go by many names: Infusion reactions (even if injected), IRRS, IRS, anaphylactoid, pseudoallergy, and more.
The industry cautioned against using these lipids (and the emulsifiers) in vaccines and injectables (one-size-fits-all therapies), as found in medical literature throughout this lipid transport and emulsifier lipid shell and liposome drug delivery history. These reactions are named repeatedly in the literature, but it is highly specified in cancer and specialty medicine, which was not well-known to the broader medical community.
For instance, here is a little information on DOXIL. DOXIL is a cancer drug from 2007 that uses the PEGylated lipid PEG2000, the same PEGylated lipid in the mRNA Covid-19 injections. Please take note of the adverse reactions in the box section below. Also, note what the drug manufacturer points to as the potential cause of the anaphylaxis reactions: the liposomal lipids. These early PEGylated drugs were so toxic that they had to be infused over several weeks’ time and at one-and-a-half-hour infusions, and pre-treatment with steroids and/or other pretreatments (to help prevent unwanted reactions) were required for the infusions.
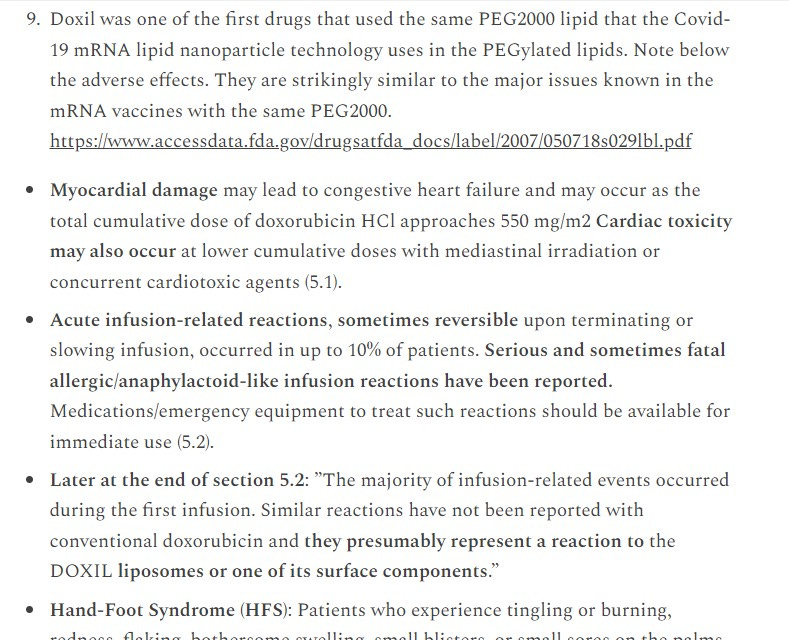
Please go to the DOXIL webpage for more information.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/050718s029lbl.pdf
Take a look just above and then go to the FDA DOXIL website to see the black box warning at the top of the page. I am sure you also noted the myocardial issues; I see them too, but the drug maker doesn’t say what the caused them as they did with the anaphylactoid (AKA pseudoallergy) reactions.
Anaphylaxis and anaphylactoid reactions are not mild or nominal reactions, and anaphylactoid reactions (also known as infusion reactions (even if injected)) can sometimes have delayed reactions up to months. Yes, months. Per the EMA, the lipids can stay in the body for up to four months.
Please speak to a medical professional who is knowledgeable about pseudoallergy, anaphylaxis, and lipid reactions that can take place with certain drugs, food additives, contrast dies, latex, and more. I am not a physician, so please talk to your physician to verify and to learn from him or her about these reactions and their causes. If your physician is not familiar with these reactions or the lipids, keep looking for one that is. Then, double-check them.
Again, I am not a doctor, but a systemic reaction from the Covid-19 injections nearly killed my son.
His reaction did not happen in the first half hour, the day of, or days after his injection. But his case is diagnosed and documented, and his antibodies point directly at the lipid shell. He also did not have a history of PEG allergy, nor was he diagnosed with PEG allergy. One of the top minds in mRNA medicine, Dr. Robert Malone, describes delayed reactions in his videos and writings, as well as describes PEG as likely being the cause of the sudden deaths that happen shortly after injections. I don't say these things to be a bit more than others.
I am begging you not to let this happen to you or to your children. Read my son’s story, or read the story of our friend’s son Junior, who died at age 16, just five days after his injection.
Voluminous textbooks are currently used in our medical colleges that teach immunologists and physicians in relevant fields of medicine to understand, diagnose, and look for adverse reactions and immunotoxicity from nanoparticle drugs.
The following is found in the book, “Immune Aspects of Biopharmaceuticals and Nanomedicines” (Jenny Stanford Series on Nanomedicine), “This text provides a thorough understanding of immunology, therapeutic potential, clinical applications, adverse reactions, and approaches to overcoming immunotoxicity of biotherapeutics and nanomedicines.” This is one example. There are many. I have a copy of a few of these books; they are the largest textbooks I own.
However, general practitioner medical doctors only receive a little, if any, exposure to these teachings unless they seek it out. It is a newer technology, and this is the first time the LNPs have been administered in an injection worldwide. But please know that if books the size of three Bibles exist to teach about these issues, there is much to learn.
Deadly Astroturf :
What is frightening is that astroturf-style (fake grassroots marketing to confuse facts and sell ideas or products) cigarette company playbook marketing is aimed at confusing even the medical industry about PEG and PEGylated lipids in injections and infusions. “Big business” will do big things to protect their money, so you are most likely unaware of the full details about PEG, PEGylated lipids, and the past of PEGylated liposomal drugs. In the case of the COVID-19 injections, the NIH, FDA, and drug manufacturers spent billions of dollars on this “clean-up” of the SARS-CoV-2 virus in the form of the COVID-19 “vaccines,” to be paid by you, the taxpayer, but they are likely getting hundreds of billions back in return (in one form or another). They likely care about that money above . https://www.scientificamerican.com/article/for-billion-dollar-covid-vaccines-basic-government-funded-science-laid-the-groundwork/
Astroturf: This link provides an excellent ten-minute video on astroturfing. In the professional world (especially medicine and politics), astroturf or astroturfing is widely used to influence opinions and purchases. Astroturf: Manipulation of media messages, fake articles, medical papers, television media, and even social media accounts that are all made to look as if they come from genuine sources or even are an individual or grassroots movement, but in fact are marketing tactics by large marketing firms. See Sharyl Attkisson – TEDx University of Nevada:
“The big business of nanomedicines had an estimated value of US$53 billion in 2009. The industry is projected to reach a total market value of approximately US$334 billion by 2025… The major portion of nanomedicine market revenue is for therapeutics, consisting of drugs, devices, and drug delivery systems.
” https://www.futuremedicine.com/doi/10.2217/nnm-2019-0130
With these pandemic drug pushes, censored drugs, and failed policies, we have seen grifting and astroturfing on a global level. My hope is that many now realize that we need to take a very close, microscopic look at what took place during the pandemic. We must use critical thinking, look at the reason, ask for the details and consider that there is more than meets the eye. The money will tell us the truth; the LNPs are worth hundreds of billions. The Spike protein is not valuable to them. It got them their EUA to get the LNP passed.
Please remember that Dr. Fauci’s wife head’s up the Drug Approval
Please remember that even though the frontline doctors were successfully treating the virus, the FDA began approving EUA authorizations for new drugs and for the Covid-19 vaccines, saying that the drugs the frontline doctors used were not effective, even though, as Dr. B says, these Washington organizations like the FDA and CDC directors never treated a single Covid-19 patient.
The below-linked “ZS” article, “Understanding COVID-19 treatment development timelines”, describes the work that was being done early on in the pandemic to approve treatments such as antivirals and monovalent drugs. All the treatments on this page are novel treatments or repurposed treatments, and all require Emergency Use Authorization: dated October 2020.
https://www.zs.com/insights/understanding-covid-treatment-development-timelines
[On the date of this writing, many were never approved, and of the few that were approved, some had their EUA withdrawn (details can be found here on the FDA page). https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization#coviddrugs ]
The “ZS” article explains, “Treatments that further reduce both morbidity and mortality, however, remain an unmet medical need.”
And this is how we ended up with the EUA for the Covid-19 “vaccines.” The multitudes of already FDA-approved drugs didn’t protect people from “morbidity” and “mortality” (according to the FDA, as they went forward with EUA drugs instead), and the “vaccine” and drugs that they approved with Emergency Use Authorization were meant to meet this need. Let’s find out if they did.
We know that these EUA drugs met the FDA’s financial need for sure.
The Players, Contracts & Playbook:
We already see what Pfizer is up to in the pandemic, as I wrote of the leaked FDA OIC email above. I may add more information about Pfizer, but I already know quite a bit about them as they use the same dangerous lipids in the LNP shell that Moderna does, the one that nearly took my son’s life. His case study is in pre-print but may be published by the time some of you read this article. I also have articles about this technology’s issues in my Substack.
So, let’s find out what Moderna was up to during the Pandemic. To me, it looks like Moderna was in the “right place at the right time,” ready with technology in record time: “Moderna produced a vaccine within six weeks. The first patient was vaccinated in an NIH-led clinical study on March 16; early results from Moderna’s 30,000-volunteer late-stage trial showed it was nearly 95% effective at preventing COVID-19. “ (link below. That is astounding, both the speed and the efficacy claims, as the “vaccines” are now known to show much different results in both reduced efficacy and alarming morbidity rates (but more on that later).
But maybe these claims are not so astounding when I read (from my point of view) that Moderna essentially IS the NIH, it seems, where the Moderna Covid-19 vaccines are concerned, or at least they are intertwined, but you can decide with what was written in the November 2020 Scientific American article (link below) that discusses the money and the relationships with Moderna and the NIH as it starts with some of the history of the parties and their twists and turns therein,
“Graham, now deputy director of NIH’s Vaccine Research Center… In 2016, Graham, McLellan, and other scientists, including Andrew Ward at the Scripps Research Institute, advanced their concept further… and a patent was filed for its design by NIH, Scripps, and Dartmouth…. NIH and the University of Texas—where McLellan now works—filed an additional patent...”
As stated further in the article, “Although other scientists have advanced proposals for what may be even more potent vaccine antigens, Graham is confident that carefully designed vaccines using nucleic acids like RNA reflect the future of new vaccines.”
Next, “Graham’s NIH lab, meanwhile, had started working with Moderna in 2017 to design a rapid manufacturing system for vaccines… The Moderna vaccine,… emerged directly out of a partnership between Moderna and Graham’s NIH laboratory.”
“…Graham’s boss at NIH, Anthony Fauci, highlighted the spike protein work.” Found in the Scientific American Article: For Billion-Dollar COVID Vaccines, Basic Government-Funded Science Laid the Groundwork: Much of the pioneering work on mRNA vaccines was done with government money, though drug makers could walk away with big profits- November 18, 2020, https://www.scientificamerican.com/article/for-billion-dollar-covid-vaccines-basic-government-funded-science-laid-the-groundwork/
If I am looking at this correctly, Graham, (the pandemic-era NIH Deputy Director), who designed aspects of the Moderna Covid-19 vaccines, went to work with the NIH, the work went with him, and Dr. Fauci became his boss. Next, Dr. Fauci then pushed these vaccines and promised they were effective. Does this seem like a conflict of interest?
It is hard to follow the many twists and turns in these relationships. But we should ask, should the head of the NIH have pushed a “vaccine” that he was in charge of and oversaw the development of, onto the public with an EUA? Above, the article explains how other scientists had advanced proposals. I’m paraphrasing, but it indicates that these advanced proposals were overlooked in favor of the “vaccine” that Graham and Dr. Fauci were overseeing.
Although they claim in the article that “Under a 1980 law, the NIH will obtain no money from the coronavirus vaccine patent. How much money will eventually go to the discoverers, or their institutions isn’t clear. Any existing licensing agreements haven’t been publicized; patent disputes among some of the companies will likely last years. HHS’ big contracts with the vaccine companies are not transparent…”
Further in the Scientific American article, “Coronavirus vaccines are likely to be worth billions to the drug industry if they prove safe and effective …” And shockingly goes on to say, “If, as many scientists anticipate, vaccine-produced immunity wanes, billions more doses could be sold as booster shots in years to come. And the technology and production laboratories seeded with the help of all this federal largesse could give rise to other profitable vaccines and drugs.”
So, it seems they are saying that if they are effective, they make billions and if they are not effective and the immunity wanes, “billions more would be sold in years to come” as booster shots, then this will lead to more money in more “vaccines” and drugs with this technology.
Again, this tech struggled for approval for years and only saw approval through an EUA. This should greatly concern you and bring you to demand answers.
Remember Christine Grady, Dr. Anthony Fauci’s wife, and NIH’s chief bioethicist. It seems that the world was looking at her relationship with the approval process for the Covid-19 vaccines. Much of the NIH and FDA denied that the NIH had anything to do with drug approval.
So, the world began to look into that, including the filing of FOIA (Freedom of Information Act) requests. An Epoch Times Article entitled, “ NIH Officials Ignore FOIA Request for Details of Fauci’s Wife’s Health Agency Job” By Mark Tapscott, Updated: July 19, 2022, states, “Grady is listed on the NIH website as “Senior Investigator” and “Chief of the Department of Bioethics at the National Institutes of Health Clinical Center.” Her title is currently listed by the U.S. Office of Personnel Management as “Social Science” with a pay level of $238,970, according to data compiled by Open the Books. The current top pay rate for federal government executive-level officials is $226,300. https://www.theepochtimes.com/nih-officials-ignore-foia-request-for-details-of-faucis-wifes-health-agency-job_4603776.html
Then I began to look into that. Let’s go back to this NIH document written Wednesday, February 24th, 2010 (at the dawn of biomedicine), entitled, “NIH and FDA Announce Collaborative Initiative to Fast-track Innovations to the Public Partnership Combines Strengths to Speed New Treatments to Patients”.
That is interesting. This article goes on to show the 2010, newly developed relationships connected with biomedicine within the NIH and FDA ( written before the censorship of the pandemic reared its ugly head). In this article, it states, “As part of the effort, the agencies will establish a Joint NIH-FDA Leadership Council to spearhead collaborative work on important public health issues. The Joint Leadership Council will work together to help ensure that regulatory considerations form an integral component of biomedical research planning, and that the latest science is integrated into the regulatory review process.”
“In addition, the NIH and the FDA will jointly issue a Request for Applications, making $6.75 million dollars available over three years for work in regulatory science. The research supported through this initiative… will inform the scientific and regulatory community about better approaches to evaluating safety and efficacy in medical product development.”
Additionally, it states, “The effort will rely on the NIH's vast experience supporting and facilitating new discoveries in the laboratory and clinic, and the FDA's more than 100 years of experience and knowledge in the regulation and approval of drugs, biologics, and medical devices.”
It goes on, "The FDA plays an essential and unique role in how therapies are evaluated. We are the bridge between biomedical research discoveries and new medical products," said Margaret A. Hamburg, M.D., Commissioner of Food and Drugs. "We now have a special opportunity—and responsibility—to harness advances in science and technology to support our efforts. We are working in collaboration with the best minds and research institutions available so that we can better develop and utilize new tools, standards and approaches needed to properly assess the safety, effectiveness and quality of products currently in development or already on the market."
It continues to say, "For more than two decades, the NIH and the FDA have been partners in many initiatives designed to improve the health of millions of Americans," said NIH Director Francis S. Collins, M.D., Ph.D. "This collaboration, however, is the first of its kind and will use the NIH’s breadth of experience as a leader in biomedical sciences to help make the translation of biomedical discoveries into effective treatments as seamless as possible." https://www.nih.gov/news-events/news-releases/nih-fda-announce-collaborative-initiative-fast-track-innovations-public
So, to catch us up, if I follow all of this correctly, in 2010 the NIH and FDA aligned, and biomedical research was given a multi-million dollar boost in the arm to get the project off the ground; the LNP shell was already in design and in the works (according to the article above on Moderna). Through this Dr. Fauci is head of NIAID within the NIH, and his wife is the chief Bioethicist. Then Dr. Fauci brought Graham (the pandemic-era NIH Deputy Director), who designed aspects of the Moderna Covid-19 vaccines, to work in that role within the NIH. The vaccines are given a warp speed EUA approval.
Many in the news and the country are concerned with the speed of the “vaccine” roll-outs and the relationships involved (especially given the global failures seen in these “vaccines” and the policies set out by these agencies). How did the vaccines get their EUA? I’m not sure many trust answers from the NIH, the CDC, or the FDA now.
Part of the issue is that when FOIA requests are filed to look at these relationships, the NIH ignores them. When Brook Jackson (Regional Director with a company named Ventavia Research Group, whose work was to oversee the conduct of Pfizer's Phase 3 Covid-19 mRNA "vaccine" trial at several locations in Texas), files a complaint to look further into her concerns, “I felt that I had a responsibility to make sure that the participants were protected and that the fraudulent data being collected in the study was not used in any safety and efficacy analysis” ( https://www.iambrookjackson.com/ ).
It is clear that these issues need to be thoroughly investigated, but by who? Who could or would be trusted to investigate at this point?
[Look below for more of the money trail and as we learn the details of how the LNP shell (used in other drugs besides the “vaccines”) is already bringing in the money found in the “Shell Game” and the “Grift Within the Shell Game.”]
Did the FDA, the CDC, and the NIH Ignore Efficacy?
How does efficacy or failed efficacy potentially tie into the relationships and the EUA?
Take note of this bullet point from the October 2020 “ZS” article, Pharmaceuticals and Biotech/ Understanding COVID-19 treatment development timelines.
“Imperfect efficacy: The U.S. Food and Drug Administration (FDA) is requiring COVID-19 vaccine developers to demonstrate that their candidate is at least 50% more effective in preventing disease than placebo—even at full vaccination where transmission is reduced, the virus may remain in circulation.”
https://www.zs.com/insights/understanding-covid-treatment-development-timelines
As the world has been seeing greater reports of reduced efficacy, in these vaccines, with the vaccinated making up more death and illness than the unvaccinated, in a just world, it would make sense that this FDA requirement for the drug manufacturers would necessitate the Covid-19 vaccines to be re-evaluated, putting the EUA authorization in question, and perhaps withdrawing it, as was done for the numerous non-vaccine biological products described above in the ZS and FDA article which shows that all but two of the first drugs were withdrawn as they don’t work with the new variants.
But consider these words spoken by “Dr Rochelle Walensky, a physician-scientist who directs the US Centers for Disease Control and Prevention (CDC) and Dr William Powderly, an infectious diseases physician from Washington State, expressed reservations about the current enthusiasm for Covid vaccination: “So many of us wanted to be hopeful: this [vaccination] is our ticket out. Now we are done”. Looking back, they say there was “too little caution and too much optimism.” We skated over the possibility of resistant variants. Walensky and Powderly concluded that “the science was grey, not black and white.” Found in the Quadrant Online article, “COVID Vaccines’ Biomechanics and Efficacy,” 20th March 2022 by Robert Clancy (Emeritus Professor of Pathology at the University of Newcastle Medical School). https://quadrant.org.au/opinion/public-health/2022/03/a-briefer-on-covid-vaccines-biomechanics-and-efficacy/
Although I feel that this is a softball swing at the issue and does not hit hard at the admission that the Covid-19 vaccines are not effective, it at least has an acknowledgment that they are indeed not effective and acknowledgment that there was “too little caution.”
So, here we read the admission of reduced efficacy from the CDC director, and if one looks, one can find words from the NIH, Dr. Fauci, who has been known to express that the Covid-19 vaccines have questionable (my word as I am paraphrasing) efficacy.
With this, I wonder if we have not seen this efficacy issue re-visited with the Covid-19 “vaccines” because of the tight relationship between Dr. Fauci, the NIH, and Moderna outlined above in the “Billion Dollar Covid-19 Vaccine…” article by Scientific American. After all, they had the plan to make money if they were effective, and they had the plan to make money even if they were not effective (booster shots). So, it looks like they had no plan surrounding efficacy.
I write quite a bit about some of the science behind failed efficacy in my other articles; there are at least three mechanisms for potential built-in failed efficacy within these “vaccines.”
But it would seem that these agencies can’t now, nor could not at any point in the past, acknowledge failed efficacy as the EUA would be withdrawn and, with it, the “Billion Dollar Baby.”
The Shell Game:
The lipid shell LNP, their “Billion Dollar Baby,” poised to bring hundreds of billions to the LNP developers in other drugs:
Understanding the Spike Protein, The mRNA Payload, and The Platform-
“In discussing the dangers within the Covid-19 “vaccines,” it is important to note that there are known inflammatory responses to the mRNA “vaccine’s” spike protein. Scientists and physicians also point out that other potentially harmful impurities and anomalies may also be found in the Covid-19 vaccines.
In my writing, I focus on the lipid shell or “platform” of the mRNA Covid-19 “vaccines” as they contain a known toxin that was shown to be harmful before the Covid-19 vaccines were developed, and this lipid shell is the “Billion Dollar Baby” that I refer to often as it will likely be around much longer than the payload or the spike protein payload or center.
The lipid shell is the aspect of the mRNA technologies that presented significant problems which kept this technology from gaining access to approval in the past. There were many years of work on this lipid nanoparticle technology, but it had been found to be too toxic and problematic to progress to a stage where it would see FDA approval without the Emergency Use Authorization allowing it into use in the pandemic. The lipid shell is called LNP (or lipid nanoparticle), mRNA shell or LNP shell, etc.
A little reading on this issue about the struggle to get LNP drugs onto the market can be found in my article “The Shot Heard Around The World” and my article “Do we already have our answer? Reduced efficacy of the mRNA vaccines and altered drug distribution in the body”,
Also see this very important information can be seen here in the article, “Lavishly funded Moderna hits safety problems in a bold bid to revolutionize medicine’ which states, “But mRNA is a tricky technology. Several major pharmaceutical companies have tried and abandoned the idea, struggling to get mRNA into cells without triggering nasty side effects.
Bancel has repeatedly promised that Moderna’s new therapies will change the world, but the company has refused to publish any data on its mRNA vehicles, sparking skepticism from some scientists and a chiding from the editors of Nature.”
In my opinion, this quote does above not fully address the startling reason why these pharmaceutical companies abandoned the idea of getting mRNA into cells, but this is a start, found in “STAT news online,” Damian Garde, Jan. 10, 2017, https://www.statnews.com/2017/01/10/moderna-trouble-mrna/
Also, this December 2020, science.org article was written when the Covid-19 mRNA vaccines came to market and began showing the same anaphylactic issues seen with the lipid nanoparticles in the previous attempts with these lipids in human drugs. The article, “Suspicions grow that nanoparticles in Pfizer's COVID-19 vaccine trigger rare allergic reactions - Life-threatening responses seen in at least eight people could be linked to polyethylene glycol, known to trigger reactions to some drugs”, shows Pfizer and Moderna’s early pandemic, December 2020, maneuvering as the PEGylated lipids and the lipids in the vaccine shell showed to be a known issue within the Covid-19 mRNA vaccines, tipping safety red flags within NIAID.
Note that according to the article, these dangerous PEG issues were discussed in both financial and several NIAID (National Institute of Allergies & Infectious Diseases) meetings.
Also found within this science.org article, “Life-threatening responses seen in at least eight people could be linked to polyethylene glycol, known to trigger reactions to some drugs,” further, we read, "Nevertheless, the companies were aware of the risk. In a stock market prospectus filed on 6 December 2018, Moderna acknowledged the possibility of "reactions to the PEG from some lipids or PEG otherwise associated with the LNP." And in a September paper, BioNTech researchers proposed an alternative to PEG for therapeutic mRNA delivery, noting: "The PEGylation of nanoparticles can also have substantial disadvantages concerning activity and safety.'"
"Others are skeptical of the [PEG] link. Still, the U.S. National Institute of Allergy and Infectious Diseases (NIAID) was concerned enough to convene several meetings last week to discuss the allergic reactions with representatives of Pfizer and Moderna, independent scientists and physicians, and the Food and Drug Administration (FDA)."
Again, much more writing on this subject can be found within my Substack online and below, as well as information can be found in my presentations and interviews that Dr. B and I have taken part in. I provide information that is hard to find in this article, which discusses how PEG and PEGylated lipid reactions are more than allergic reactions, many articles will state they are allergic reactions, and I think that is dangerous as people can die from PEGylated lipids without having a PEG allergy. So, how can I not take my time to write this, knowing my son was not diagnosed with a PEG allergy and had not had a PEG reaction before, but nearly died from the mRNA lipid shell? See the story on his vaccine injury for more information.]
So what is the Shell or platform? The lipid shell is the outer portion of the mRNA drug delivery technology and is also called the platform. I call it the “Billion Dollar Baby”.
The center, the inside portion of the mRNA technology, is called the “payload,” which is contained within the lipid shell (where the spike protein is housed in the Covid-19 “vaccines”).
The payload can be manufactured with different medications or vaccine “payloads” inside the shell/platform.”
One way to think of the technology is like a round chocolate with a filling inside. The chocolate outer portion represents the lipid shell, and the inner portion can have a filling (caramel, for instance). The filling portion is the payload, and for Covid-19 mRNA “vaccines,” the spike protein is part of the payload, housed inside the lipid LNP shell.
In manufacturing the lipid shell drugs or vaccines, the payload can be changed out for other drugs or medicines.
Again, the spike protein is found in the “payload,” and the lipid shell is the “platform.”
Another way to think of this technology is to think of the shell/platform as a bubble and the payload as the open area that can be filled with contents inside the bubble.
Other drugs/medications (payloads) can be encased inside a lipid shell (bubble) in LNP therapeutics for other types of vaccinations and treatments
I have been thorough about this as the platform/the lipid nanoparticle LNP shells (outer portion) is about to be used in numerous vaccines and treatments, representing billions of dollars for the drug companies, but the lipid nanoparticles contain toxic PEGylated lipids that can harm more people than the industry may be willing to admit.

Credit: Genevant Sciences Shown is a siRNA LNP [A lipid nanoparticle (LNP) contains hundreds of small interfering RNA (siRNA) molecules, each surrounded by ionizable lipids, phospholipids, and cholesterol. The outside of the particle is coated in PEGylated lipids.
LNPs for messenger RNA (mRNA) are made with similar ingredients but contain only a few mRNA strands.]
Found here, https://cen.acs.org/pharmaceuticals/drug-delivery/Without-lipid-shells-mRNA-vaccines/99/i8 , “Without These Lipid Nanoparticles, there would be no mRNA vaccines for COVID-19- Fragile mRNA molecules used in COVID-19 vaccines can’t get into cells on their own. They owe their success to lipid nanoparticles that took decades to refine”: By Ryan Cross March 6, 2021 | A version of this story appeared in Volume 99, Issue 8
The Grift Within the Shell Game:
“A shell game is a swindle, a fraud, especially one in which items or information are shifted around in a secret manner to avoid detection. Methods of shifting money between corporations and banks to avoid taxes is an example of a shell game.”, found on Grammarist.com
Much of the focus in the pandemic has been on the Spike protein, and I understand why, in my opinion, no part of the vaccine was safe.
The spike protein causes its share of unfathomable issues, and it has been detected in autopsies, and is associated with ADE; it is thought to be at the root of the myocarditis vaccine injuries, and other significant vaccine injuries. From all that I have seen, it is not safe, and I have my opinion on why it was used in the Covid-19 vaccines.
I recognize that there are significant problems with the spike protein being added to the payload of the mRNA “vaccines.” We must remember, though, that the SARS-CoV-2 - Covid-19 virus should quiet down at some point. It may not, though, given the way that our world of modern medicine has been orchestrated. In the world, we knew pre-pandemic pandemics had never been known to last forever. Let’s pray that this one isn’t manipulated to last forever.
If the novel viruses of the past tell us anything, the spike protein should fade away for some time. Hopefully, that will give dedicated and moral scientists time to research it properly.
The money trail continues to tell me that the real prize and motivation in much of the pandemic by the drug companies and the entities that held an interest in the pandemic is the LNP shell/ lipid drug platform.
My friend, who has become one of the leading advocates worldwide for safe drugs and pharmaceuticals, always says to follow the money. Below I will highlight the rest of the twisted money trail that many may not have seen the underbelly of during the pandemic. It should shock you or at least concern you and bring you to speak out and discuss these matters so that every detail is exposed. We should demand it.
In the November 2020 ZS, article cited above, it is made clear that the technology was lying in wait for the ability to go forward. This is described stating the LNPs “finally get their chance to shine” in reference to the EUA.
The quest for this LNP shell to find its way into multi-millions of households tells a tale that is far more surreal than fiction can conjure up. However, this story is not my story; it is spoken in the language of peer-reviewed medical journal articles and papers; it tells a tale that is told by many, and it spans over 20 years. I will bring these cases, articles, and findings to light as we journey into the Billion Dollar Baby.
As we read about the issues seen in the LNP over twenty years, we should keep asking why those that designed and saw a potential use for the LNP shell/platform could not, after more than 20 years, attain approval for the lipids to be used in injectables, that is, without the Emergency Use Authorization (EUA) enacted in the sars-Cov-2 (Covid-19) pandemic.
Also, consider that the pharmaceutical companies Moderna and Pfizer struggled to obtain approval due to the known issues surrounding PEG and PEGylated lipids pre-pandemic. Yet, billions of dollars of drug contracts flooded in when, during the pandemic, with its gaining the EUA (Emergency Use Authorization), the LNP shell quietly gained approval for two bio lab companies. Yes, two bio lab companies gained approval of the LNP shells that never went through proper testing and trials. See more information in ”Who Is Dr. Malone Substack”, “mRNA Vaccines Fact Versus Fiction,” October 27th, 2022:
So, I asked my friend, who is the world’s leading global drug safety advocate, who has spent the last 19 years working and speaking out about potentially harmful drugs, and who speaks in presentations and media across the globe, why the LNP shell (which never went through proper trials and approval), is now allowed usage by these drug manufacturers in emerging drugs, and why did the LNP shell not go through new drug trials for the new drugs. She explained that once an aspect of a drug has gained previous approval, it is not required to gain new approval in new drug usage. Apparently, that even applies to EUA, which astounds me and should astound you as well.
The importance of my asking this is because the LNP shell never went through the proper stages of drug trials, efficacy, and safety testing, as it was approved during the EUA, but it is now approved for use and is in LNP flu shots and will be in the LNP child vaccines in the vaccine schedule, and the issues with PEG and the lipids were never resolved.
But you may not know this information if you read many of the articles written on the subject once the pandemic began.
Many of these pandemic-era articles about the LNPs and PEG or PEGylated lipids feel as if they have a slant to them. I believe a good portion of them are Astroturf (discussed earlier: false grassroots media & stories that look and feel like news but are developed and distributed by marketing firms to sway consumers, voters, etc.).
These articles are similar in that they feed the public a little information about the possible “reactions” seen in PEG-containing, LNP, or lipid-containing drugs and products but then “walk it back” or minimize the potential harms with other points of view and propaganda that feel quite a bit like the cigarette industry campaigns of the ’50s through the ’70s.
In my opinion, especially post-pandemic, immune, and anaphylactic concerns with PEG and nano lipids are rarely appropriately addressed in media that discusses PEG or PEGylated lipids, or nano lipids. Since the pandemic arrived, discussions about PEG or PEGylated lipids typically appear in the news, with caveats often stating that one must be allergic to PEG or have PEG antibodies to be harmed.
This is not the case according to numerous pre-pandemic findings and discussions within the medical literature (some of this literature is funded or written by or with the inclusion of the drug companies themselves). PEG2000 and the lipids didn’t suddenly become safer somehow; in fact, the pre and pandemic-era PEG used in these drugs that I speak of and that are in the Covid-19 “vaccines” is the same PEG2000 configuration of the nano lipid used in the Covid-19 mRNA shells (AKA platform).
To be clear, life-threatening, and life-ending anaphylaxis can occur in those who are not allergic to PEG as PEGylated lipids do unusual things in our immune system, described in full below, where I discuss CARPA and the ABC phenomenon and something that I call the “antibody one-two punch.” Again, in Covid-19 vaccination injuries and reactions, we are seeing a mirror to the reactions seen in the early PEG and lipid drugs that took place pre-pandemic. This research and data are worth a thorough exposure as they show 20-plus years of documentation. That history cannot be erased in favor of creepy, mad-men cigarette-style advertisements disguised as medical information articles in magazines, not medical journals.
From what I see, there has been an intense effort to promote and push the pharma industry’s “cleaned up“ media version of its billion-dollar baby (PEGylated LNP shell) with these astroturf distractions over the accurate and full picture of the harms (which are life-threatening and life-taking), so that questioning the use of the LNPs was delayed until they could gain their approval, which they have.
Now, consider that with the PEGylated lipids /LNP in circulation in the population via the Covid-19 “vaccinations,” the spike protein has been reported to cause nearly identical reactions to PEG and PEGylated lipids that are injected or infused (seen in the linked article above “COVID Vaccines’ Biomechanics and Efficacy” and the article below “Microthrombosis Is the Main Cause of Death.”
The PEGylated lipid reactions will not have suddenly disappeared because they went through an EUA, so they logically will continue to be seen. This, of course, will be to a certain percentage, and then (even according to the “astroturfed” accounting of the issues seen in PEGylated lipids) to a more significant percentage of people as PEG antibodies (which are known to cause the below Allergic reactions and CARPA type reactions) will have now been developed in a staggering number of individuals who have received the Covid-19 mRNA injections.
With this, keep in mind that the Emergency Use Authorization (EUA) for the “vaccines” could not occur if drugs were available that met the need for efficacy in Covid-19 infections. There would be no need for it. So, the propaganda and “campaigning” for the “safety” of this LNP formulation was big business. We should demand to know who received funds from the CDC, NIH, FDA, et al. for advertising expenditures during the pandemic. We should be shown every ad that we pay for as taxpayers. I haven’t found it. Most likely, many will direct me to this information. If they do, I will update this article to get it to you.
In closing, it appears that sitting solidly within this grift is the story of promising existing and emerging drugs that were “overlooked” during a global pandemic tells part of this bigger story of greed and of drug companies doing what they are now notoriously known for, pushing more expensive or, in this case, more expensive, more controversial, and more invasive drugs no matter the cost to human lives. We will look at these drugs just below.
Were Alternate and Alternative Therapies Gaslighted and Overlooked Within the Shell Game:
To catch us up to here, we have learned about the EUA (emergency use authorization), and its importance, and we have met the parties involved in seeing the “vaccines through to achieve its “EUA,” and their relationships. We have seen the money involved, the ignored FOIA request, and the OCI’s involvement, as stated in the Epoch Times article, which lays out their findings on Brook Jackson’s complaint being ignored by the FDA.
Then, we see how the lipid shell (LNP) is beginning to bring billions of dollars in revenue for the parties that are set to benefit; we see how the same agencies tried and failed to get the LNP approved due to safety concerns but that it was done anyhow through the EUA (emergency use authorization within the CDC). We also see how the “vaccines” have efficacy issues. We are all aware of the safety issues, including Pfizer and Moderna, who are doing their own studies on the adverse reactions and who now have “Myocarditis” warnings on the drug labels.
Now we will look closer at the apparent gaslighting of the alternative therapies and treatments that could have been potentially used in the pandemic to save lives. We will also look at the reason why this was important and how the EUA continues to be pivotal and vital to these issues.
To start, please know that when I say medications that were “alternate therapies,” I’m not just speaking of the alternative treatments that you probably have some knowledge of, such as ivermectin and hydroxychloroquine; those were absolutely cast aside and had their names dragged through the mud (so shameful, but there is more to the story). You should also know of the potential, safer options that our CDC, FDA, and NIH did not consider.
I came across research about a couple of SARS-CoV-2 prohibitors (nasal sprays) showing that Covid-19 can potentially be halted in the body. They began development during the pandemic. I have also looked at promising intranasal vaccines that do not use mRNA technology, injections, or PEGylated lipids. However, I have seen spike protein used in these vaccines, so I will focus on the prohibitors as I know most people are rightfully thinking about safer alternatives that don’t involve toxins and gene therapies for future medications. Everything needs to be questioned from here on out.
This is why when I saw these studies and emerging therapies, one of my first thoughts was, “who is going to trust new medications after what we have been through in the pandemic?” I also thought, who will trust any recommendations by the CDC, the NIH, and the FDA? I’m not asking these questions alone. The agencies themselves are asking how to regain public trust; just look at Brook Jackson’s case and the OCI involvement.
So, our country is questioning how we might look at new ways of approving drugs for the market as the FDA as we know it and the giant public health agencies failed, as we have seen in the pandemic. Or at least they do not work in the current configuration that we know them now. Similar failures are known in the NIH, as evidenced by the recent “change up” in command in the NIH and numerous articles on this subject.
To regain the public’s trust in the giant public health organizations, if that is possible, these agencies would possibly have to be re-formed, re-vamped, and perhaps even disbanded in favor of a more cooperative citizen-led private sector watchdog group for approving drugs. What this would look like would take the minds of many with expertise in the development of pharmaceutical drugs and take far more discussion than can be accomplished here, but the most important aspect should be that the voice of the people would have a place in determining the safety and efficacy of new drugs, as well as complete transparency in these processes.
It would be incredible for citizens to see a real-world ability for any concerns in the upcoming drugs to be addressed through transparent, definitive answers, solutions, and/ or the denial of drug approval completely as needed.
So, assuming that our country has a new, re-vamped FDA or FDA-like ability to assure safety and effectiveness in medications, vaccines, and drugs, I’d like to show you these interesting SARS-CoV-2 prohibitors (nasal sprays) (with one in use now in labs to keep the mice and rats from getting Covid-19 infection).
Most people know about ivermectin, hydroxychloroquine, and the monoclonal antibodies, but these interesting SARS-CoV-2 prohibitors (nasal sprays), EK1C4 and EKL1C arrived on the scene during the pandemic. With further trials and studies, they (or any number of intranasal spray-formulated potential therapies and nasal vaccines (providing that they do not include spike protein or PEG or PEGylated lipids)) could have been considered as part of the EUA drugs that saved lives. With proper investigation and trials, they possibly could have been used as primary therapy or treatment in the Pandemic in place of the Covid-19 ‘vaccines” in a more rational world. The links and more information on these prohibitors are below towards the end of this article. Also, the following linked article at the end of the next paragraph provides information and cites interesting links on this subject.
Why is this important? Because you can’t inoculate a mucosal disease with a parental vaccine, so says a battery of information from epidemiologists and medical studies. Consider the following, “Mucosal immunity is a key compartment in our immune system, different from the antibody response in the blood that's stimulated by vaccine shots,” said Michael Mina, an epidemiologist and chief scientific officer for at-home testing company eMed. According to the article “Why we need to be talking about vaccines that offer "mucosal immunity," written by Tina Reed, on September 13th, 2022, found here: https://www.axios.com/2022/09/13/why-vaccines-mucosal-immunity-covid
Here is another article, with important reading about mucosal compartment infection, found in the article “COVID Vaccines’ Biomechanics and Efficacy”, which states, “The primary objective of this essay is to discuss the immunology of COVID-19 and its response to vaccination. If we accept COVID is a mucosal compartment infection, we can see why repeated unspaced vaccination can backfire. Many years of repeated infection by coronaviruses that we encounter along the way establishes a state of regulated immunity with respect to the pandemic variant, COVID-19. Natural immunity and, to a greater extent, vaccine-induced immunity are limited. There is always the risk of dominant immune suppression, a risk amplified by repeated antigen stimulation.
Current data from many countries point to promotion of infection in subjects exposed to compressed booster programmes. Experience with allergy desensitisation points to the risk of long-term immune tolerance serving to compromise anticipated seasonal vaccination programmes for COVID.” Robert Clancy (Emeritus Professor of Pathology at the University of Newcastle Medical School; He is a member of the Australian Academy of Science’s COVID-19 Expert Database), written on March 20th, 2022, found here: https://quadrant.org.au/opinion/public-health/2022/03/a-briefer-on-covid-vaccines-biomechanics-and-efficacy/
So, understanding that these intranasal therapies and SARS-CoV-2 prohibitors are emerging topics in the world of coronavirus’, I want to talk about the prohibitors as they don’t have mRNA gene therapy or spike protein in them, and for the prohibitors that I looked into, the “secret sauce” is derived from pomegranate peel, yes, and wait until you read how it works. I find it promising that in their progression and development, the second prohibitor, brings up important issues of safety that were left out of the equation in the Covid-19 vaccines and that I know to be life-threatening.
I want to know more. I also continue to wonder why our government suppressed some drugs and/or overlooked the drugs that were already in development of potential, non-invasive, effective treatments against Covid-19, in favor of the mRNA LNP Covid-19 vaccines. Is it possible that their billion-dollar baby (LNP shell, lipid platform) was more important than human lives?
The above Axios article touches on this idea as well in many areas of the article, but here are two solid examples, “But the U.S. isn't putting money into such products, which experts say could augment current vaccines on the market.” And “Late last month [August 2022], Senate Republicans sent a letter to the Biden administration calling for an Operation Warp Speed-like project for intranasal vaccines to reduce transmission, as well as pan-coronavirus approaches.”
These agencies certainly were clear in telling the physicians which drugs to use and not use during the pandemic; why not discuss these intranasal drugs and the development of intranasal mucosal therapies? Now in late 2022, the white house claims the money is all used up, and there are no more funds to invest in these possibilities.
The CDC and NIH spell out information on each of their “approved drugs list,” heck they even made a meme that a horse could understand when unjustly and insidiously censoring and “suggesting” against ivermectin.
I believe that failing to declare the Covid-19 vaccines unsafe and ineffective while ignoring drugs that either already had the ability to address the Covid-19 infection or were emerging and had the ability to do so as well; this caused an unknown level of harm to our population and society.
Let’s look at some of the emerging alternatives:
As I bring you these findings, know that I am acutely aware of the many that say that we should have all just endured Covid-19 and survived it with current medications that we already knew to reduce viral load, and address inflammation, blood clotting, and autoimmune responses in the body.
I couldn't agree more, but aside from Ivermectin (which I have extensive research and writing on as well), I’ll show that there were at least a couple of other potential therapeutic responses that could have been legitimately explored to address the SARS-CoV-2 virus. There are a few more, nasal application therapies within the articles linked on the page above.
I know from first-hand experience that ivermectin worked for me as a co-therapy (with zinc), but I also saw it work in a more serious case, as it helped a family member who was already struggling for his life when he contracted Covid-19. With Ivermectin used as a co-therapy with Zinc, his case showed extensive improvement on the two occasions that he was treated with ivermectin. Keep in mind, though, that even though it worked so well for this family, not all drugs work for all people. This is why a single ailment may have many treatments to choose from to address it.
We should still continue to ask why known effective and inexpensive drugs were not recommended or allowed to be used in Covid-19 cases by the major hospitals and by way of decrees from the CDC.
Some of the non-vaccine therapies that saw the discovery and work towards development during the pandemic derive from pomegranate peel that has been developed with the goal of prohibiting the Covid-19 virus in humans and in one therapy that is successful in doing so in mice and rats in labs, meant for use in their work with mice to prevent SARS-CoV-2 in bio labs. These discoveries are intranasal sprays that have the potential to address the Covid-19 virus without injection and without spike protein.
Looking into these potential therapies, one of the potential alternative prohibitor therapies in development is a dePEGylated therapy that again, is said to use natural components of pomegranate peels. DePEGylated means that they made this therapy without the use of PEG or PEGylated lipids.
It is interesting that the word DePEGylated was coined. It tells me that we may see more medications with these words on their labels or in their descriptions. They are distancing themselves from PEG, and they explain why within their clinical article.
The first three links below include these two potential SARS-CoV-2 inhibitors/prohibitors. The first is a link to the actual EK1C4 product that is sold now as a potential SARS-CoV-2 prohibitor for lab rats and mice, for use only in labs that work with coronaviruses, “Intranasally applied EK1C4 protects mice against HCoV-OC43 infection [1]. This lipopeptide has thus the potential to be developed as a pan-coronavirus prophylactic or therapeutic, alone or in combination with neutralizing anti-Spike antibodies.”
Please note that this science and emerging technology is provided for information to show you the development of these prohibitors, which are currently used in mice. These Pan coronavirus prohibitors describe potential use in humans. EK1C4’s “successor, or younger cousin,” EKL1C (has taken steps towards this safety as well as omitting PEG from its formulation.) I can’t know the safety involved in these drugs in their final stages, but these drugs are added to show the possibility of better solutions for medicine.
The third link below is a similar SARS-CoV-2 prohibitor proposed for use in humans that has taken further steps in safety. This article gives an explanation of why they removed PEG from the formulation. Then the fourth link below is the reference found in the citation that they use to explain the importance of refraining from the use of PEG in the potential prohibitors. This information in the 4th link is extremely important and, to me, a "smoking gun" if you look closely enough at the information given. Many will clap back at me with a knee-jerk reaction about PEG being just an allergy. They most likely have not done the research. Minimizing the potential for harm and death is not honest nor safe; it is negligent.
Again, people can die from PEGylated lipids without having a PEG allergy. So, how can I not take my time to write this, knowing my son was not diagnosed with a PEG allergy and had not had a PEG reaction before, but nearly died from the mRNA lipid shell? (See the story on his vaccine injury in my other writings for more information.)
The following two links provide information on the first of two interesting intranasal applications, SARS-CoV-2 inhibitors/prohibitors, that I will describe herein. This prohibitor derives from pomegranate peel (more information below). This first EK1C4 is included to provide a little history as I believe its successor, EKL1C, the dePEGylated version is a far safer option for the potential prohibition of coronaviruses without a systemic, injected drug and without the known antigen/allergen PEG as injected as a PEGylated lipid and without the novel protein/antigens such as spike.
What I find interesting and tangible in this information is that these articles introduce possible and potential ways to prohibit (or inhibit) the SARS-CoV-2 virus. This is the link for the actual EK1C4 product that a lab supplier sells for biolabs that work with mice and rats to prevent SARS-CoV-2 in their rats and mice in their work. Again, this is for biolabs and for mice and rats, please, don’t mistake this for a current human drug, it is a biolab product.
https://www.invivogen.com/ek1c4
Here is a 2020 article that discusses the prohibitor’s success and ease of use (as an intranasal spray). As found in the link below, “EK1C4 is expected to be safe to humans because it will be used locally, not systemically, and peptide drugs are generally safer than chemical drugs. Fifth, because of its broad-spectrum anti-coronavirus activity, EK1C4 can be used for treatment and prevention of infection by not only SARS-CoV-2 but also other HCoVs.” https://www.nature.com/articles/s41422-020-0305-x
I personally know that reactions to PEGylated lipids can be life-threatening, and PEGylated lipids are used in this formulation, EK1C4 (linked just above). As such, the information on EK1C4 is given only to show the progression of this technology.
Below, is the link and information for the DePEGylated answer to EK1C4 (aimed at prospective human dosing). This drug is named EKL1C and the information is found in a study done in 2021 that describes this SARS-CoV-2 prohibitor, which eliminates the known allergen/antigen immunogenic PEG from its formula/ingredients and is a less invasive (nasal spray) answer than injections for potentially inhibiting the SARS-Cov-2 virus. This prohibitor also derives from pomegranate peel.
Again, given the multi-billions of dollars that have been available in Covid relief funds and government research grants allocated for this global health crisis, such a prohibitor, or one like it, could potentially have been given priority for research and development, but it was not, and this may be for a host of reasons. But we should consider looking at these numerous promising, potentially less harmful therapeutic answers to Covid-19 infection, especially given the continued, alarming Covid-19 “vaccine” reports of death and injury.
The article on EKL1C, “A highly potent and stable pan-coronavirus fusion inhibitor as a candidate prophylactic and therapeutic for COVID-19 and other coronavirus diseases”, by Jia Zhou et al. written on April 4th, 2022, can be found here: https://www.sciencedirect.com/science/article/pii/S2211383521002756#bib45
This fascinating article in Frontiers in Science called, “Pomegranate Peel Extract as an Inhibitor of SARS-CoV-2 Spike Binding to Human ACE2 Receptor (in vitro): A Promising Source of Novel Antiviral Drugs”, goes into the use of the pomegranate peel further, “For centuries, humans have used plant extracts for medicinal and beneficial health purposes, even though the active compounds responsible for the extract efficacy were mostly unknown. There are thousands of examples of the use of plant-derived compounds as drugs, nutraceuticals, and cosmetic ingredients.” Thank you, Annalisa Titi et al. and Arterra Bioscience SPA, Naples, Italy, for publishing this work, dated 08/21/2021, found here: https://www.frontiersin.org/articles/10.3389/fchem.2021.638187/full
Again, the EKL1C SARS-CoV-2 prohibitor not only derives from Pomegranate peel, but it also has no harmful PEG or PEGylated lipids in it. Found within the link and “highly potent pan-coronavirus fusion inhibitor…” article above that described the scientist’s concerns with PEG in their formulation, "However, recent studies have shown that some PEG-modified therapeutics could induce PEG-specific antibodies in vivo, resulting in decreased therapeutic efficacy40, 41, 42, 43. It was also reported that PEG conjugation at the C-terminus of a lipopeptide could enhance its sensitivity to proteolytic enzymes18,44. Most recently, it was reported that at least eight health volunteers who received the mRNA COVID-19 vaccine produced by Pfizer and BioNTech suffered severe allergy-like reactions, possibly because these people may have had high levels of the preexisting antibodies against PEG, which was used in the nanoparticles for mRNA packaging of the vaccine.
Therefore, to circumvent these limitations, we designed and synthesized eight dePEGylated lipopeptides by replacing the PEG linker with some amino acids ...
The Importance of excluding PEG or PEGylated Lipids in Vaccines & Therapies: PEG- Pfizer, Moderna and NIAID Knew and They Did Not Tell Us-
Most importantly, the dePEGylated lipopeptide EKL1C exhibited significantly stronger resistance to the proteolytic enzymes, trypsin, and proteinase, better metabolic stability in mouse sera, and higher thermostability than the PEGylated lipopeptide EK1C4, suggesting that our strategy offers a possible solution to the limitations of PEG linkers in PEGylated drugs. Since the dePEGylated lipopeptide EKL1C contains no PEG, it is unlikely to cause severe allergy-like reactions in people who have high levels of the preexisting anti-PEG antibodies." Found in the above-dePEGylated lipopeptides article "...prophylactic and therapeutic for COVID-19 and other coronavirus diseases".
Of importance, in the EKL1C article, the drug maker’s concerns with using PEG, were referenced and detailed in the below article detailing Pfizer and Moderna’s early pandemic, December 2020, maneuvering when they were informed that the PEGylated lipids and the lipids in the vaccine shell were a known issue, tipping red safety flags within NIAID. Note two things, one is that Dr. Fauci became director of NIAID in 1984, and two, that these dangerous PEG issues were discussed in both financial and several NIAID (National Institute of Allergies & Infectious Diseases) meetings. Found within the Science.org link below, in the article
“Suspicions grow that nanoparticles in Pfizer's COVID-19 vaccine trigger rare allergic reactions: Life-threatening responses seen in at least eight people could be linked to polyethylene glycol, known to trigger reactions to some drugs”, written Dec 21st, 2020, By Jop de Vrieze, and with some quotes repeated from page eleven due to importance:
"Nevertheless, the companies were aware of the risk. In a stock market prospectus filed on 6 December 2018, Moderna acknowledged the possibility of "reactions to the PEG from some lipids or PEG otherwise associated with the LNP." And in a September paper, BioNTech researchers proposed an alternative to PEG for therapeutic mRNA delivery, noting: "The
PEGylation of nanoparticles can also have substantial disadvantages concerning activity and safety.'"
"Others are skeptical of the [PEG] link. Still, the U.S. National Institute of Allergy and Infectious Diseases (NIAID) was concerned enough to convene several meetings last week to discuss the allergic reactions with representatives of Pfizer and Moderna, independent scientists and physicians, and the Food and Drug Administration (FDA)."
They went ahead with them anyhow.
Fauci is the head of National Institute of Allergy and Infectious Diseases NIAID as the Director within the NIH. Let that sink in.
To me, this article does not hit hard, nor does it explain possible crossover reactions and the life-threatening and life-taking nature of the reactions seen in PEG-related anaphylaxis, CARPA, or the potential reactions they mention from "the lipids," which would include, of course, phospholipids and the cationic lipids that many have spoken of.
Note in this article (regarding the antibodies) the one-two punch within the Covid-19 shots that I talk about in my work and interviews: Here, the first PEGylated lipid injections trigger antibodies to PEG, and then the second injection can trigger an anaphylaxis reaction to PEG or PEGylated drugs. Now consider the boosters given in this scenario, knowing the potential dangers therein. Again, where were you NIAID?
Next, the information below, which discusses the dangers of the lipids/PEGylated lipids & liposomal drugs and LNPs, will sound familiar as they mirror some of the life-threatening and deadly issues seen in the current vaccine injured.
Reminder: The vaccine manufacturers are now investigating their own drugs, which I believe is a conflict of interest if they expect society or the FDA to accept their reports on the adverse reactions at this point, especially given the knowledge of how the FDA and Pfizer “handled” Brook Jackson’s concerns (discussed through this article).
These reactions and dangers, and warnings are not new. We have seen it before. The quote below is from an article from 2015, pre-pandemic (linked below).
"...and that this activation can lead to the binding of these cells to each other and also to capillary endothelial cells, entailing
microthrombus formation and circulatory blockage, mainly in the pulmonary and coronary microcirculation."
"In essence, CARPA may be perceived as biological stress on blood that arises as a consequence of the similarity of nanomedicines to viruses, between which the immune system cannot make difference (8). The entailing acute inflammatory reaction may have triple harms via 1) causing rapid clearance of the drug and, hence, reducing or eliminating its efficacy: 2) causing an acute illness in the host whose most severe manifestation is anaphylaxis: and 3) leading to immunogenicity, which turns drugs into vaccines and thus abolishes their therapeutic use (9, 10)." Found in the article, “Blood cell changes in complement activation-related pseudoallergy” written by Zsófia Patkó and János Szebeni/ Found in the European Journal of Nanomedicine: https://doi.org/10.1515/ejnm-2015-0021
I would add, argue, or ask that if in its reduced efficacy, this leaves the "vaccine" essentially ineffective, and what remains from exposure and injection of the “vaccine” only the potential or realized damages to the body?
Remember that the EUA for these “vaccines” hinged on efficacy.
So, again, take note of this bullet point from the December 2021 article, “Imperfect efficacy:
The U.S. Food and Drug Administration (FDA) requires COVID-19 vaccine developers to demonstrate that their candidate is at least 50% more effective in preventing disease than placebo—even at full vaccination where transmission is reduced, the virus may remain in circulation.” https://www.zs.com/insights/understanding-covid-treatment-development-timelines
Further, this article, Anatomical and Pathological Observations and Analysis of SARS and COVID-19, https://pubmed.ncbi.nlm.nih.gov/33472576/: Microthrombosis Is the Main Cause of Death, is added to point out that known issues/adverse reactions seen in the LNPs mirror life-threatening diseases natural covid infection.
Why would this be? We need to ask loud and clear why a “vaccine” would be developed and approved by EUA that had toxins known to cause life-threatening and life-taking reactions. The toxin had the known potential to produce mirrored reactions to the natural SARS-Cov-2 Covid-19 viral infection and nearly identical reactions to the utilized payload antigen, the spike protein. Ask yourself and ask others why this would be. Then follow the money.
That is the Billion Dollar Baby’s Billion Dollar Question.
Heather Hudson
I am not a doctor, and all that I write is not meant to diagnose or treat any condition. I also do my best to give the source of the information that I find to you. I say this as I give this information for one reason, my son nearly died and I do not want to see any person, any mother, and father, brother, sister, uncle, or child to go through what my son went through and what I went through with my child clinging to life for months, it was intense, and it broke pieces of us and changed us forever. Every participant in this book has said they want to save lives.
Brief Descriptions:
ABC phenomenon: Accelerated Blood Clearance - rapid blood clearance, altered drug distribution in the body, and reduced efficacy with repeated doses (a phenomenon known to occur with lipid drugs).
CARPA: (Complement Activation- Response Pseudo Allergy (response known to occur with lipid drugs).)
DNA: for controlling the synthesis of proteins, although in some viruses, RNA rather than DNA carries the genetic information.)
DOXIL: (early PEG-containing cancer drug).
Liposomal: (According to cancer.gov, liposomal means, “A drug preparation that contains the active drug inside very tiny, fat-like particles.”)
LNP: (lipid nanoparticle -nanoscopic fat particle).
mRNA: (messenger RNA (According to Oxford Languages, ribonucleic acid, is a nucleic acid present in all living cells. Its principal role is to act as a messenger carrying instructions from
PEG: (polyethylene glycol).
Pharmacokinetics: The branch of pharmacology concerned with the movement of drugs within the body.
Pharmacologists: Medical scientists working to develop new drugs. They may work in a lab, testing medications by studying tissue and cell samples
SARS-CoV-2: The virus that causes Covid-19 infection.
Hi! A reader sent me here
1) I know multiple people who developed anaphalaxis after COVID vaccination. Despite this, none of them were able to get a medical exemption.
2) Antiphospholipid syndrome seems to be a major issue with these vaccines. I wrote more about it here:
https://amidwesterndoctor.substack.com/p/critical-thinking-in-the-age-of-censorship
Love that you're doing this, what would be good would be if some of the key info were packaged into smaller amounts or a link to that info so that we can repost on places like twitter e.g. the info on the LNP never being tested and now becoming part of the vaccines in the childhood schedule as if I post such a long thread, I doubt people would read through it